|
Overview
 The most common cause of heel pain is plantar fasciitis which is commonly referred to as a heel spur. Plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, from the heel to the toes. Plantar fasciitis is a condition in which the plantar fascia is inflamed. This condition can be very painful and cause a considerable amount of suffering. Causes Some of the many causes of heel pain can include abnormal walking style (gait), such as rolling the feet inwards. Obesity. Ill-fitting shoes. Standing, running or jumping on hard surfaces. Injury to the heel, such as stress fractures. Bursitis (inflammation of a bursa, bursae are small sacs that contain fluid to lubricate moving parts, such as joints and muscles). Neuroma (nerve enlargement). Certain disorders, including diabetes and arthritis. Symptoms Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment. Diagnosis The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders. Non Surgical Treatment If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain. Surgical Treatment It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation. how to get rid of heel spurs Prevention  Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs. Overview
 Babies are often born with flat feet, which may persist well into their childhood. This occurs because children?s bones and joints are flexible, causing their feet to flatten when they stand. Young babies also have a fat pad on the inner border of their feet that hides the arch. You still can see the arch if you lift your baby up on the tips of the toes, but it disappears when he?s standing normally. The foot may also turn out, increasing the weight on the inner side and making it appear even more flat. Causes There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape. At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side. Symptoms Most patients who suffer from flat feet or fallen arches often do not complain of any symptoms whatsoever. However, on some occasions, patients may find that their feet are fatigued fairly easily and following activity on long periods of standing may have a painful foot or arch. On occasions, swelling may be seen on the inner aspect of the foot and performing certain movements may be painful and difficult. Some patients who have flat feet may find that their feet tend to roll in (over-pronate) a lot more when they walk and run. As a result, they may experience damage to the ankle joint and the Achilles tendon, as well as excessive shoe wear. Diagnosis If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination. What does it mean when you have flat feet? Non Surgical Treatment There are different modalities of treatment that are available to manage flat feet and fallen arches. The type of treatment that is chosen depends upon how severe the condition is and what symptoms the patients are experiencing. Below is a brief description of the available treatment modalities. In the event that the patient is experiencing swelling of the feet, rest and ice application is usually the initial treatment step. Oral anti-inflammatories may be offered which can help reduce inflammation as well as associated pain. Physical therapy has good outcomes and can include different exercises such as stretches and strengthening of the surrounding muscles. Changes in footwear and activity modification are also important when dealing with a painful flat (pronated) foot. These days, orthotic insoles are easily available either over the counter or through your Podiatrist which can effectively help maintain the arch of the foot and reduce the amount of stress placed on the foot. Podiatrists are able to prescribe a variety of different devices from prefabricated to customized and are trained to determine the most appropriate device for each individual. In order to offer the right kind of orthotic insole, podiatrists may perform a test called gait analysis. This involves asking the patient to walk and videoing the different movements that the foot of forms during the walking. Features such as over pronation can be easily seen on this and orthotic insoles can be prescribed to correct the specific abnormalities that are picked up on this analysis. Overall, orthotic treatment can result in a significant improvement in foot movement and reduction in foot discomfort. Surgical Treatment  Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low. Overview
Having one leg shorter than the other is a common physical condition. It has two primary causes--structural or functional problems. Structural differences in length can be the result of growth defect, previous injuries or surgeries. Functional differences in length can result from altered mechanics of the feet, knee, hip and/or pelvis. These altered mechanics from functional leg length discrepancy often stem from having an unbalanced foundation.  Causes The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions. Symptoms The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result. Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment Heel lifts and sole lifts are simple ways Pedorthists can compensate for leg length deficiencies. These small modifications can make a tremendous difference to a person?s comfort, balance and mobility. Although people do not always know if they have LLD if you have any of the symptoms I have mentioned you should consult a Pedorthist as treating your condition early will reduce the development of serious problems later on.  how to increase height fast in 1 week Surgical Treatment Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces. Overview
 Morton's neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton's neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton's neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton's neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary. Morton's neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton's neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton's neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton's neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.Causes Although the exact cause for this condition is unclear, a number of factors can contribute to the formation of a neuroma. Biomechanical deformities, such as a high-arched foot or a flat foot, can lead to the formation of a neuroma. These foot types bring on instability around the toe joints, leading to the development of the condition. Trauma can cause damage to the nerve, resulting in inflammation or swelling of the nerve. Improper footwear that causes the toes to be squeezed together is problematic. Avoid high-heeled shoes higher than two inches. Shoes at this height can increase pressure on the forefoot area. Repeated stress, common to many occupations, can create or aggravate a neuroma. Symptoms People with Morton's neuroma usually complain of pain that can start in the ball of the foot and shoot into the affected toes. However, some people just have toe pain. There may also be burning and tingling of the toes. The symptoms are usually felt up the sides of the space between two toes. For example, if the nerve between the third and fourth long bones (metatarsals) of the right foot is affected, the symptoms will usually be felt up the right-hand side of the fourth toe and up the left-hand side of the third toe. Some people describe the pain that they feel as being like walking on a stone or a marble. Symptoms can be made worse if you wear high-heeled shoes. The pain is relieved by taking your shoe off, resting your foot and massaging the area. You may also experience some numbness between the affected toes. Your affected toes may also appear to be spread apart, which doctors refer to as the 'V sign'. The symptoms can vary and may come and go over a number of years. For example, some people may experience two attacks of pain in a week and then nothing for a year. Others may have regular and persistent (chronic) pain. Diagnosis Morton's neuroma is usually diagnosed by your doctor listening to your symptoms and examining your foot. Sometimes your doctor can feel the 'neuroma', or an area of thickening in your foot, which may be tender. Sometimes, your doctor may suggest an ultrasound scan or MRI scan to confirm the diagnosis but this is not always necessary. Some doctors inject a local anaesthetic into the area where you are experiencing pain. If this causes temporary relief of pain, burning and tingling, it can sometimes help to confirm the diagnosis and show the doctor where the problem is. Non Surgical Treatment Treatment depends on the severity of your symptoms. Your doctor will likely recommend trying conservative approaches first. Arch supports and foot pads fit inside your shoe and help reduce pressure on the nerve. These can be purchased over-the-counter, or your doctor may prescribe a custom-made, individually designed shoe insert, molded to fit the exact contours of your foot.  Surgical Treatment Surgery is occasionally required when the conservative treatment is not able to relieve your symptoms, particularly if you have had pain for more than 6 months. 80% of patients who require surgery report good results, with 71% of people becoming pain-free. Prevention It is not always possible to prevent a Morton's neuroma. However, you probably can reduce your risk by wearing comfortable shoes that have low heels, plenty of toe space and good arch support. There are two unique variations of leg length discrepancies, congenital and acquired. Congenital indicates that you are born with it. One leg is anatomically shorter than the other. As a result of developmental phases of aging, the human brain senses the gait pattern and recognizes some difference. The body typically adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch is not really uncommon, does not need Shoe Lifts to compensate and mostly does not have a profound effect over a lifetime.
 Leg length inequality goes mainly undiscovered on a daily basis, yet this issue is easily solved, and can eliminate a number of cases of back problems. Treatment for leg length inequality typically consists of Shoe Lifts. These are very reasonably priced, typically costing under twenty dollars, compared to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Lower back pain is the most widespread health problem affecting people today. Over 80 million men and women are afflicted by back pain at some point in their life. It is a problem which costs companies vast amounts of money each year as a result of time lost and productivity. Innovative and better treatment methods are always sought after in the hope of minimizing the economic impact this issue causes.  Men and women from all corners of the earth suffer from foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of reducing any pain and discomfort in the feet. Shoe Lifts are recommended by countless specialist orthopaedic practitioners". So that you can support the body in a well-balanced fashion, feet have a significant task to play. Inspite of that, it is sometimes the most overlooked zone in the human body. Some people have flat-feet meaning there is unequal force placed on the feet. This causes other parts of the body such as knees, ankles and backs to be affected too. Shoe Lifts guarantee that appropriate posture and balance are restored.  Overview OverviewA hammertoe is commonly mistaken as any type of toe deformity. The terms claw toe, or mallet toe, although technically different than a hammer toe, are commonly referred as such. The toe may be flexible with movement at the joints, or it may be rigid, especially if it has been present for a long time. With a true hammertoe the deformity exists at the proximal interphalangeal joint only. Causes Hammer toe usually affects the second toe. However, it may also affect the other toes. The toe moves into a claw-like position. The most common cause of hammer toe is wearing short, narrow shoes that are too tight. The toe is forced into a bent position. Muscles and tendons in the toe tighten and become shorter. Hammer toe is more likely to occur in women who wear shoes that do not fit well or have high heels and children who keep wearing shoes they have outgrown. The condition may be present at birth (congenital) or develop over time. In rare cases, all of the toes are affected. This may be caused by a problem with the nerves or spinal cord.  Symptoms SymptomsThe symptoms of a hammer toe include the following. Pain at the top of the bent toe upon pressure from footwear. Formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe. Diagnosis Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor hammertoes may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred. Non Surgical Treatment Inserts in your shoes can be used to help relieve pressure on the toes from the deformity. Splints/Straps. These can be used to help re-align and stretch your toes and correct the muscle imbalance and tendon shortening. One of the most common types are toe stretchers like the yogatoe. Chiropody. A chiropodist can remove calluses or corns, areas of hard skin that have formed to make the foot more comfortable.Steroid injections can help to reduce pain and inflammation. Surgical Treatment If you are unable to flex your toe, surgery is the only option to restore movement. Surgery is used to reposition the toe, remove deformed or injured bone, and realign your tendons. Surgery is normally done on an outpatient basis, so you can return home on the day of your surgery.
Overview
 More than one-third of women in America have bunions, a common deformity often blamed on wearing tight, narrow shoes and high heels. Bunions may occur in families, but many are from wearing tight shoes, and nine out of 10 bunions happen to women. Too-tight shoes can also cause other disabling foot problems such as corns, calluses and hammer toes. More than one-third of women in America have bunions, a common deformity often blamed on wearing tight, narrow shoes and high heels. Bunions may occur in families, but many are from wearing tight shoes, and nine out of 10 bunions happen to women. Too-tight shoes can also cause other disabling foot problems such as corns, calluses and hammer toes.Causes Women tend to suffer from bunions more often than men, probably because of the shoes they wear. But besides shoes, standing on the feet for long periods of time can also make symptoms of a bunion worse. Along with the bump, these bunion symptoms include pain or soreness, swelling, redness around the joint, a burning sensation or sometimes numbness. The big toe may develop calluses or not be able to move as well as it once did. Sores between the toes and ingrown toenails may also occur because of a bunion. Symptoms Bunions are readily apparent, you can see the prominence at the base of the big toe or side of the foot. However, to fully evaluate your condition, the Podiatrist may take x-rays to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don't go away, and will usually get worse over time. But not all cases are alike, some bunions progress more rapidly than others. There is no clear-cut way to predict how fast a bunion will get worse. The severity of the bunion and the symptoms you have will help determine what treatment is recommended for you. Diagnosis Your family doctor or chiropodist /podiatrist can identify a bunion simply by examining your foot. During the exam, your big toe will be moved up and down to determine if your range of motion is limited. You will be examined for signs of redness or swelling and be questioned about your history of pain. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen. A X-ray of your foot may help identify the cause of the bunion and rate its severity. Non Surgical Treatment Non-surgical treatments for bunions may include wearing shoes that fit and that have adequate toe room. Stretching shoes professionally to make them larger. Putting bunion pads over the bunion to cushion the pain. Avoiding activities that cause pain, such as being on your feet for long periods of time. Taking over-the-counter pain relievers when necessary, such as acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDS) like ibuprofen. Using ice to provide relief from inflammation and pain. Using custom-made orthotic devices.  Surgical Treatment Anyone who experiences symptoms from bunions should see a podiatrist for treatment. But you may benefit from surgery if you have any of the following. Severe foot pain that limits your everyday activities, including walking and wearing comfortable shoes. You may find it hard to walk more than a few blocks (even in athletic shoes) without significant pain. Chronic big toe inflammation and swelling that doesn?t improve with rest or medications. Toe deformity, a drifting of your big toe toward the small toes. Toe stiffness, inability to bend and straighten your toes. Failure to obtain pain relief from anti-inflammatory drugs. Failure to substantially improve with other treatments such as a change in shoes and anti-inflammatory medications. Prevention Make better shoe choices. If you?re a woman, avoid high-heeled footwear whenever possible (at the very least, choose shoes with heels lower than two inches), and make sure all your footwear has a wide, deep toe box. Whether man or woman, if you?re trying on shoes and your toes feel ?squished? or crowded by a particular shoe, reject that style and try another, or go for a larger size. You don?t need to invite trouble. In general, shoes that come to a point at the toe are bad news, as they tend to push the toes together into an overlapping pattern. Shoes with rocker soles will unload pressure on the bunion area. Examine your feet regularly. Note any redness, swelling or discoloration. Flex your toes and check for any stiffness. If there is any, think back to what you?ve worn or done in the past few days. If the condition persists more than a few days, or worsens, a visit to the podiatric physician is in order.
Overview
 A bunion is an enlargement of bone at the great toe joint. Tight shoes don't cause bunions, but they can aggravate them. Bunions are often inherited and become worse over time if left untreated they can cause pain, swelling, skin irritation and other foot problems. Bunion deformities are often part of a more generalized problem related to improper foot motion. There are presently over 25 types of bunion procedures performed today. The choice of procedure is based on many factors. A bunion is an enlargement of bone at the great toe joint. Tight shoes don't cause bunions, but they can aggravate them. Bunions are often inherited and become worse over time if left untreated they can cause pain, swelling, skin irritation and other foot problems. Bunion deformities are often part of a more generalized problem related to improper foot motion. There are presently over 25 types of bunion procedures performed today. The choice of procedure is based on many factors.Causes Women traditionally have a higher rate of bunions, which is to be expected, since it is they who have traditionally worn shoes with high heels, a narrow toe box, or whatever fashion dictates from year to year. However, men can suffer from bunions as well, as can anyone for whom the right (or wrong) conditions exist, poor foot mechanics, improper footwear, occupational hazards, health and genetic predisposition. Finally, bunions have long been a condition associated with the elderly, and although they often appear in conjunction with inflammatory joint diseases such as arthritis (which is often associated with age), they can strike at any point in life, including adolescence. Symptoms symptoms and problems caused by bunions include pain. You may then have difficulty walking due to pain. Inflammation and swelling at the base of the toe. This sometimes becomes infected. The foot may become so wide that it can be difficult to find wide enough shoes. You may get arthritis in the big toe. The second toe can become deformed. In severe cases, the big toe can push your second toe up out of place. Diagnosis Most patients are diagnosed to have bunions from clinical history and examination. However, in some cases, X-rays will be performed to determine the extent of damage to the joint. Furthermore, it will enable the treating doctor to decide on the best course of management of the patient. Non Surgical Treatment A hinged flexible bunion splint, can relieve pain by providing corrective arch support and releasing tension away from the inflamed joint. Change shoes! Avoid flip flops, high-heels and shoes with pointed, narrow toe-boxes. Medicine will not prevent or cure bunions. However, the use of over the counter anti- inflammatory medications can help. Bunion splints, pads and arch supports can help redistribute weight and move pressure away from the big toe.  Prevention The best protection against developing bunions is to protect and care for your feet every day. Avoid tight and narrow-fitting shoes. Limit your use of high heels. Wear comfortable shoes with adequate space between your longest toe and the end of the shoe. Getting treatment for very flat or very high-arched feet (if you are experiencing symptoms) will give your feet the proper support and help maintain stability and balance.
Overview
One of the most common causes of arch pain is plantar fasciitis, a condition that involves inflammation of the fibrous band of tissue that connects the heel to the toes (the plantar fascia). Pain from plantar fasciitis can be felt in the arch or the heel, and is most often felt toward the end of the day and after long periods of being stationary (e.g. getting up after sitting for a long time). Commonly, plantar fasciitis is the result of excessive foot pronation (rolling in of the foot) or excessive foot supination (e.g. high arches), both of which can increase tension on the plantar fascia. In these cases, orthotics and well-fitting footwear can address the cause of the problem by improving the position of the feet and relieving tension on the plantar fascia.  Causes There are a number of other medical conditions that can cause foot arch pain such as diabetes, arthritis and obesity. These can affect the position and strength of the bones, muscles, ligaments and tendons, leading to bottom of foot pain. It sounds simple but footwear plays an important role in how our feet feel. Foot arch pain is commonly caused by ill-fitting shoes, especially ones with little arch support or that are too tight. Footwear is particularly important if you are going to be spending long periods on your feet or for sporting activities such as running. Shoes should be supportive, comfortable, cushioned, provide the appropriate level of arch support and be the correct width. Symptoms Symptoms of arch pain and arch strain are found in the underside of the foot, where the foot arch is. Arch pain and arch strain is actually inflammation of the tissue in the midfoot, formed by a band that stretches from the toes to the heel. The arch of the foot is needed for the proper transfer of weight from the heel to toe. When the band forming the arch of the foot or plantar fascia becomes inflamed, it becomes painful to perform simple tasks. Diagnosis Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods. Non Surgical Treatment The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist. In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed. Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery.  Surgical Treatment As with most surgeries, patients and physicians should consider the surgery only after other, less invasive treatments have proven unproductive. Indications for surgery include Pain. Inability to function. Failure to improve after a six-month course of specific, directed physical therapy. Failure to improve after using arch supports, orthotics, or ankle and foot bracing. Once patients are at that point, the good news is that the procedure has considerably better outcomes than more traditional flat foot surgery. In the past, surgeons would realign and fuse the three hind joints, which would cause patients to lose motion, leaving them with a significantly stiff hind foot, With these newer procedures, if the foot is still flexible, surgeons can realign it and usually restore a close-to-normal or functional range of motion in the joints. Stretching Exercises Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Overview
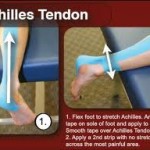 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears. An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms Symptoms of an Achilles tendon rupture usually directly follow a traumatic event where the foot is forced in an upward position at the ankle, causing a sudden tight stretch of the Achilles tendon. There can also be a direct blow to the tendon causing a rupture. There is typically a popping feeling or even a popping sound described during the occurance of the rupture. Typically there is pain with swelling in the region. Often the patient is unable to put weight on this foot as there is too much pain. Diagnosis In order to diagnose Achilles tendon rupture a doctor or physiotherapist will give a full examination of the area and sometimes an X ray is performed in order to confirm the diagnosis. A doctor may also recommend an MRI or CT scan is used to rule out any further injury or complications. Non Surgical Treatment To give the best prospects for recovery it is important to treat an Achilles' tendon rupture as soon as possible. If a complete rupture is treated early the gap between the two ends of the tendon will be minimised. This can avoid the need for an operation or tendon graft. There are two forms of treatment available for an Achilles' tendon rupture; conservative treatment and surgery. Conservative treatment will involve the affected leg being placed in a cast and series of braces with the foot pointing down to allow the two ends of the tendon to knit together naturally.  Surgical Treatment Surgery could allow for a quicker healing time. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the tissue, the repair may be reinforced with other tendons. As with any surgery, the main complication is the risk for infection, however, this risk is reduced by using smaller incisions. Prevention You can help to reduce your risk of an injury to your Achilles tendon by doing the following. When you start a new exercise regime, gradually increase the intensity and the length of time you spend being active. Warm up your muscles before you exercise and cool them down after you have finished. The benefit of stretching before or after exercise is unproven. However, it may help to stretch your calf muscles, which will help to lengthen your Achilles tendon, before you exercise. Wear appropriate and well-fitting shoes when you exercise. |
